After attending the Paris International Coccyx symposium recently I decided to post our revised approach in the light of the latest information from world experts. The system by and large follows that of JY Maigne and Doursanien who have researched this problem for many years.
Initial consultation
After taking a comprehensive history, physical examination will include:
Examination of lumbar spine and sacroiliac region to exclude causes of referred pain.
Inspection of sacrum and coccyx for lumps, bumps, sinus and dimples.
External palpation for tender sites and points
Internal examination per rectum to examine pelvic floor muscles for tension areas and trigger points in muscles. Inhibitory pressure on the offending muscles can be applied immediately to bring quick relief.
Palpation of coccyx segments and joints for local tenderness.
Assessment of mobility into flexion and extension
Diagnostic ultrasound to identify posterior shelf, subluxed segments, and dorsal spicule or bursa.
If there has been recent trauma and X ray may be taken. If more serious pathology is suspected an MRI will be ordered.
At this first consultation if an abnormal joint or a dorsal spicule has been identified you may be offered an injection under ultrasound guidance.
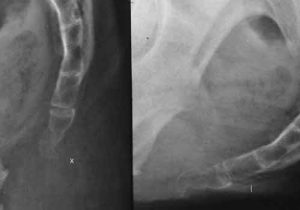
This is useful to identify subluxing (displacing segments), excessive motion into flexion or extension, calcification or rigidity.
Following this an injection into the joint above the subluxed segment will be given under XR or US guidance. If this works well it may last for a year or more. If it gives only short term relief a course of prolotherapy to strengthen the ligamentous system will be offered.
If the spicule becomes symptomatic again further injections can be given up to a limit of 3, followed by education on unlading to coccyx for several months. Useful advice on living with it, prevention and unloading can be found on www.coccyx.org

Ganglion of impar block
Just in front of the coccyx lies a small nerve ganglion ( a nest of networking vessels which marks the termination of the sympathetic chains running down the front of the spine)
Sometimes local treatment to the coccyx doesn’t work at all or is inappropriate because the cause lies in the front of the coccyx or has somehow created a deeper disturbance in the central nervous system. Under X Ray guidance a fine needle can be guided between the joints of the coccyx and after injection of radio contrast material a blockade with anaesthetic can be administered which can lastingly reset the nervous system to a normal balance.
Surgery
Sometimes the problem of severe subluxation can only be managed by surgical excision of the segments, sometimes the whole coccyx with 76% success rate. This is also the treatment for refractory dorsal spicule.
Aftercare
Losing weight, standing rather than sitting, stand up desks and PC set ups, cut out cushions, director’s chairs, building up gluteal muscles, pelvic floor training are among the many resources and directions we can employ both short and long term to prevent recurrence and improve the situation.
Dr John Tanner